
ABOUT PLASMINOGEN DEFICIENCY TYPE 1 (PLGD-1)
With PLGD-1, plasminogen levels are too low and the plasminogen that is present doesn’t work as it should.3
Plasminogen is an important protein that helps break down blood clots and heal wounds.3
PLGD-1 is associated with soft or firm, wood-like growths that can form on organs throughout the body, including the nose, mouth, lungs, and more.3
PLGD-1 is a genetic disorder that can be inherited. If you or a loved one has been diagnosed, close relatives should be tested for PLGD-1, too.2,4
Plasminogen deficiency type 1 symptoms and signs
 PLGD-1 affects the
PLGD-1 affects the entire body3
people with PLGD-1 have lesions
in multiple organs.5
Eyes
Eyes
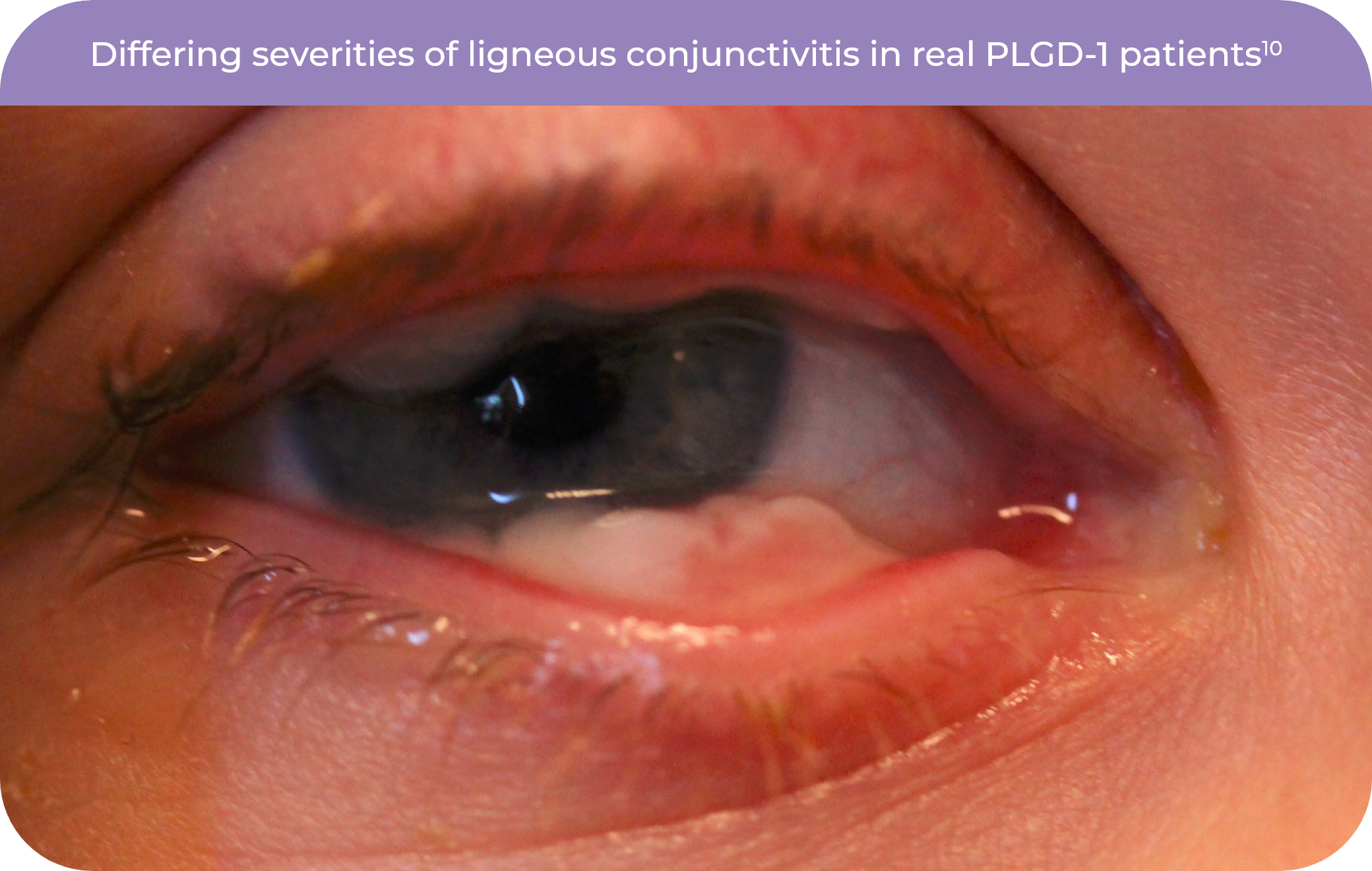
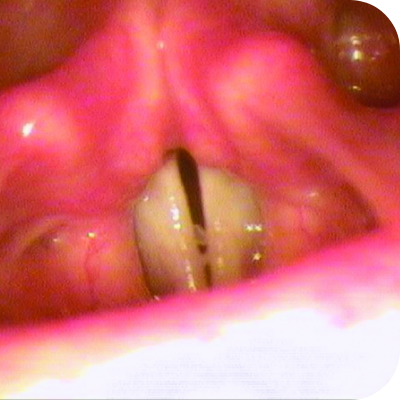
Ligneous conjunctivitis may look similar to pink eye or other common eye problems. Lesions may look firm, slimy, or mucousy and don’t improve with usual treatments. Without proper care, they can damage vision or may lead to blindness.6,7
Hear a real patient storyBrain
Brain
These lesions can block normal fluid flow, leading to hydrocephalus (fluid build-up in the brain).
Some people with PLGD-1 may also develop Dandy-Walker syndrome, a condition where parts of the brain don’t form as expected.2
Mouth
Mouth
Lesions on the gums are typically painless and are often described as white spots around the teeth that won’t come off. Left untreated, lesions can lead to gum and tooth loss.2
Hear a real patient storyEars
Ears
In the ear, lesions can cause pain, discharge, trouble hearing, and repeated ear infections. If not treated, they can lead to hearing loss.2,6
Hear a real patient storyRespiratory Tract
Respiratory Tract
Respiratory lesions may first look like frequent pneumonia, asthma, or a cough that won’t go away. Without treatment, they can block the airway, cause a collapsed lung, or lead to trouble breathing.6
Hear a real patient storyRenal System
Renal System
Lesions in the renal tract may cause kidney stones, blockages, or poor kidney function. Without treatment, lesions could lead to kidney disease or kidney failure.6
Female Reproductive Tract
Female Reproductive Tract
Lesions in the female reproductive organs can cause very painful periods, irregular or missing periods, pain during intercourse, and infertility, which can make it difficult to have children.2
Hear a real patient storyGastrointestinal Tract
Gastrointestinal Tract
Lesions in the gastrointestinal tract can cause symptoms like stomach pain, blood or mucus in the stool, or ulcers, similar to inflammatory bowel disease.6,8
Learn how to test for PLGD-1Skin
Skin
When PLGD-1 affects the skin, it can cause juvenile colloid milium, which shows up as small, firm bumps on sun-exposed skin. Cuts and wounds may also heal more slowly than expected.2
Researchers are still learning how often these lesions happen in different organs. This may change as more people are diagnosed and we learn more about PLGD-1.
Lesions that don’t heal can seriously affect how organs work and a person’s quality of life9
Talk to your doctor about your treatment schedule to make sure all visible and hidden lesions are under control
PLGD-1 most commonly affects the eye, causing ligneous conjunctivitis5
87% of people with PLGD-1 have ligneous conjunctivitis.5
Ligneous conjunctivitis, or LC, is a rare form of chronic conjunctivitis that can be mistaken for constant pink eye, granulomas, or allergic conjunctivitis. LC is the most common sign of PLGD-1.6,7
With LC, unusual growths form on the inner lining of the eyelids with symptoms like discharge, constant tearing, and redness.7
Patients describe these growths as thick white eye boogers, eye drainage, and white lesions or bleeding under the eyelids.7
LC can also appear more severely with firm, thick lesions that have a wood-like texture.7
Most people with PLGD-1 have lesions in multiple organs5
Symptoms of lesions throughout the body often look like more common sicknesses like frequent ear infections or a constant cough.6 Don't miss signs of PLGD-1 throughout the body.
Lesions can look different from person to person, even in the same organ
PLGD-1 lesions range from watery and stringy to firm and wood-like. Symptoms may come and go, vary in severity, and can differ even among members of the same family.2,6
Explore image gallery

PLGD-1 can be diagnosed at any age3,5,7*



*Researchers are still learning about PLGD-1; these statistics may change as more people are diagnosed and more information becomes available.
Want to learn more about PLGD-1?
If your doctor suspects PLGD-1, they will6
Check for lesions
both inside and outside the body, as PLGD-1 impacts the entire body.
Review family medical history
since PLGD-1 is a genetic disorder.
Run a simple blood test
that measures how well your plasminogen is working.†
†Your doctor may run additional tests measuring how much plasminogen you have and/or a genetic test showing mutations in the plasminogen gene, but these are not needed to confirm a PLGD-1 diagnosis.6
If you've been diagnosed with PLGD-1, talk to your doctor to see if RYPLAZIM is right for you.
Your doctor may work together with a hematologist, someone who specializes in conditions affecting the blood.
APPROVED USE
RYPLAZIM® (plasminogen, human-tvmh) is used for the treatment of patients with plasminogen deficiency type 1 (hypoplasminogenemia).
IMPORTANT SAFETY INFORMATION
Do not use RYPLAZIM if you are a patient with known hypersensitivity to plasminogen or other components of RYPLAZIM.
- Bleeding: Use of RYPLAZIM may lead to bleeding at disease-related lesion sites or worsen active bleeding not related to disease lesions. Discontinue RYPLAZIM if serious bleeding occurs. If you are treated at a healthcare provider’s office or center, your healthcare provider will need to monitor you during the infusion and for 4 hours afterward, especially if you have a predisposition to bleeding or are taking anticoagulants, antiplatelet drugs, or other medications that may interfere with normal coagulation. If you infuse RYPLAZIM at home, you or your caregiver must also monitor you during and for 4 hours after the infusion under the same circumstances.
- Tissue Sloughing: If you have mucosal lesions in your respiratory tract, especially the tracheobronchial tree, and are treated with RYPLAZIM, respiratory distress may occur due to tissue sloughing. Please monitor appropriately.
- Transmission of Infectious Agents: RYPLAZIM is made from human plasma and therefore carries a risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent, and theoretically, the Creutzfeldt-Jakob Disease (CJD) agent. You should consult with your healthcare provider if you have any questions or concerns.
- Hypersensitivity Reactions: Hypersensitivity reactions, including anaphylaxis, may occur with RYPLAZIM. Immediately report any of the following signs or symptoms of an allergic reaction to your healthcare provider: swelling of the throat, tightness of the chest, low blood pressure, rash, nausea, vomiting, a tingling or pricking sensation, restlessness, wheezing or shortness of breath.
- Neutralizing Antibodies: Antibodies neutralizing plasminogen (also known as inhibitors) which can make the product less effective or ineffective, may form with the use of RYPLAZIM, although they were not observed in clinical trials. If clinical efficacy is not maintained (e.g., development of new or recurrent lesions), your healthcare provider will determine low levels of plasminogen in your plasma.
- Laboratory Abnormalities: Due to the activity of RYPLAZIM, you may have elevated blood levels of D-dimer that may interfere with screening for venous thromboembolism (VTE) using D-dimer levels.
- Adverse Reactions: The most frequent (incidence ≥ 10%) adverse reactions in clinical trials were abdominal pain, bloating, nausea, fatigue, extremity pain, hemorrhage, constipation, dry mouth, headache, dizziness, arthralgia, and back pain.
You may report side effects to +1(855)-353-7466 and US_Medicalinfo@kedrion.com or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
For more details, please see full Prescribing Information and the Patient Information.
This site is intended for residents of the US only.
References:
1. RYPLAZIM [prescribing information]. Kedrion Biopharma Inc. 2024.
2. Congenital type 1 plasminogen deficiency. NORD. Updated February 6, 2025. Accessed February 5, 2026. https://rarediseases.org/rare-diseases/congenital-plasminogen-deficiency
3. Schuster V, Hügle B, Tefs K. Plasminogen deficiency. J Thromb Haemost. 2007;5(12):2315-2322.
4. Mehta R, Shapiro AD. Plasminogen deficiency. Haemophilia. 2008;14(6):1261-1268.
5. Klammt J, Kobelt L, Aktas D, et al. Identification of three novel plasminogen (PLG) gene mutations in a series of 23 patients with low PLG activity. Thromb Haemost. 2011;105(3):454-460.
6. Shapiro AD, Nakar C. How I treat type 1 plasminogen deficiency. Blood. 2025;145(25):2954-2965.
7. Schuster V, Seregard S. Ligneous conjunctivitis. Surv Ophthalmol. 2003;48(4):369-388.
8. Balram B, Thiesen A, Kroeker KI. Inflammatory bowel disease: a gastrointestinal presentation of congenital plasminogen deficiency. ACG Case Rep J. 2021;8(5):e00613.
9. Shapiro AD, Menegatti M, Palla R, et al. An international registry of patients with plasminogen deficiency (HISTORY). Haematologica. 2020;105(3):554-561.
10. Data on file. Kedrion Biopharma Inc.